
































Time to revisit ‘official’ approaches to HIV?
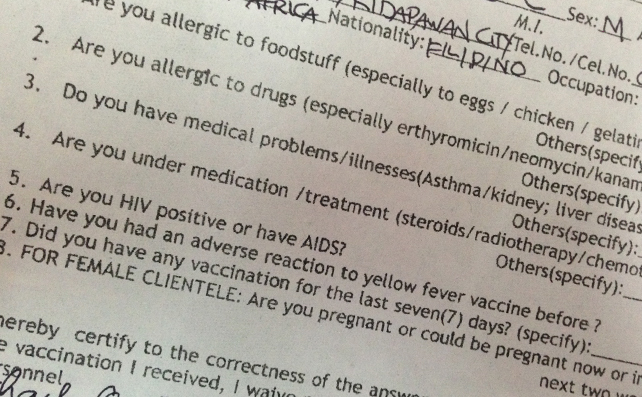
The Bureau of Quarantine’s (BOQ) form specifically states that it “encourages” those who will get the yellow fever (YF) vaccination (to get their “yellow card”, which is needed by those traveling to/from select Latin American and African countries, among others) to be “honest” to “avoid possible medical complications”. But honesty, in this case – and as relayed by a Filipino living with HIV, Xander* – came at a price.
“The first step is to fill in a form that expects one to detail his/her medical condition. This form is then checked by a nurse (the second step), who will decide if you can proceed to the third step, which is the actual vaccination. If he/she has doubts about your entries in the form, you will be sent to one of the doctors on duty; he/she will determine if you can get vaccinated,” Xander relayed to Outrage Magazine.
The problem, said Xander, is in the handling of HIV-related cases.
When he went to the BOQ in the City of Manila, first, “my filled-in form was handled by at least three people who passed it around before I was forwarded to the doctor on duty (that day).” And because this section of the BOQ did not have partitions that could have afforded him privacy, Xander deemed what happened to him as “invasive, as it failed to respect my right to privacy,” he said. “In fact, by the time I was forwarded to the doctor on duty, even the other people who were also only there to get vaccinated already knew of my HIV status.”
And then the doctor on duty “was not even familiar with HIV-related cases,” Xander alleged, basing his assumption/observation on this doctor’s “lack of knowledge about CD4 and ARV (antiretroviral medicines) – he kept saying ‘Kailangan ko yung CD-CD ba ‘yun (I think I need that CD thing)?’ and ‘Dalhin mo lahat ng gamot mo sa akin. Hindi ko masyado alam ano yang Lamivudine-Tenofovir-Efavirenz (You have to show me all your medicines. I’m not very familiar with Lamivudine-Tenofovir-Efavirenz).” The doctor’s table was, by the way, right beside the waiting area (where people who were already vaccinated were awaiting their yellow card) and the cashier (where those who get vaccinated pay for the services received), so that everything discussed was done in public.
Xander – with head hanging low – left the BOQ sans knowing that the vaccination he desired; but also shamed because of his HIV status.
HIV AND YF VACC
The doctor on duty when Xander went to the BOQ was – in a way – right to be cautious when he asked for more information about Xander’s health condition.
In a study titled “Yellow fever vaccination in HIV-infected patients”, published in HIV Therapy, Olivia Veit, Christoph Hatz, Matthias Niedrig and Hansjakob Furrer stated that “millions of HIV-infected individuals are at risk to YF, a severe hemorrhagic disease which is endemic in tropical areas of Africa and Latin America.” To deal with this, “the 17D YF vaccine (17DV) is the most effective preventive strategy.” The World Health Organization (WHO), in fact, recommends that all people aged ≥9 months living or travelling in areas where there is a risk of YF transmission to be vaccinated.
Particularly in relation to HIV, there are some things worth stressing here.
First, “data regarding safety and immunogenicity of 17DV in HIV-infected individuals are limited to small studies, mainly in travelers with CD4 cell counts above 200 cells/mm”.
Second, even with sparse information, “according to current recommendations, 17DV should only be given to asymptomatic HIV-infected individuals with a CD4 cell count above 200 cell/mm” since “rare serious adverse events cannot be excluded”. As per WHO, “the vaccine is contraindicated for people who are severely immunocompromised”.
And third, at least according to some studies, “yellow fever vaccine did not result in any serious adverse events in HIV-positive individuals. However, people with HIV responded less well to the vaccine than their HIV-negative counterparts, and the protective effects of the vaccine wore off more quickly.”
All in all, though, there is still “a special need for further studies to investigate the safety and efficacy of 17DV in HIV-infected individuals”.
Section 41 of the IRR (implementing rules and regulations) of the RA 8504 states: “Medical confidentiality shall protect and uphold the right to privacy of an individual who undergoes HIV testing or is diagnosed to have HIV.”
LAW OF THE LAND
But again, as Xander stressed, YF vaccination isn’t his issue, per se; instead, it is the handling of his situation by a government office as a Filipino living with HIV.
Republic Act 8504 (or the Philippine AIDS Prevention and Control Act of 1998, otherwise known as the AIDS Law) states (in Section 3b): “The State shall extend full protection of human rights and civil liberties to persons living with HIV.” Part of the protection clause of the existing law is ensuring that “the right to privacy of individuals with HIV shall be guaranteed.”
Section 41 of the IRR (implementing rules and regulations) of the RA 8504 states:
“Medical confidentiality shall protect and uphold the right to privacy of an individual who undergoes HIV testing or is diagnosed to have HIV. It includes safeguarding all medical records obtained by health professionals, health instructors, co-workers, employers, recruitment agencies, insurance companies, data encoders, and other custodians of said record, file, or data.
“Confidentiality shall encompass all forms of communication that directly or indirectly lead to the disclosure of information on the identity or health status of any person who undergoes HIV testing or is diagnosed to have HIV. This information may include but is not limited to the name, address, picture, physical description or any other characteristic of a person which may lead to his/her identification.
“To safeguard the confidentiality of a person’s HIV/AIDS record, protocols and policies shall be adopted by concerned officials, agencies and institutions.”
Section 44 of the IRR, in fact, details the sanctions against violators, i.e.:
“Penalties for violating medical confidentiality, as provided in Sec.s 30 and 32 of RA 8504, include imprisonment for six (6) months to four (4) years. Administrative sanctions may likewise be imposed…”
FAILURES OF THE SYSTEM
YF vaccine can only be had in three BOQ offices in the Philippines – i.e. BOQ – Manila, 25th Street, Port Area, Manila (Monday to Friday, 8am to 2pm); BOQ – Cebu, General Maxilom Avenue (Wednesday and Thursday, 8am-9am); and BOQ – Davao, Chavez St. (Fridays 8-9am).
Xander went to BOQ – Manila.
(Outrage Magazine sent on two separate dates two representatives to observe the processes of BOQ – Manila; and we can verify the same – Ed)
The BOQ “system” is somewhat different in Cebu City, still another place where the YF vaccine can be had; though there, forced HIV disclosure could still happen.
(Outrage Magazine also sent a representative to observe the processes of BOQ – Cebu; and we can verify the same – Ed)
In Cebu, people who intend to get the YF vaccine are first asked to “register”. Then those who will be given the vaccination for the first time are ushered into a private room where they are given a mini-lecture by the resident doctor re YF (and in our undercover representative’s case, sermon re HIV). During this mini-lecture, the resident doctor also asked the group if any one of them is HIV-positive. Not surprisingly, none openly admitted his (as there were only males in that batch) HIV status.
Emails were sent by Outrage Magazine to Dr. Janette L. Garin, Secretary of the Department of Health (since BOQ is under DOH), and to Dr. Ferdinand S. Salcedo, Director of the BOQ.
Specifically, Outrage Magazine sought for more information on:
- The intake forms of BOQ – e.g. if these rely on self-disclosure of HIV status, and who handles these forms since (as was reported to Outrage Magazine, these were just left on tables so that everyone could see them; and
- The set-up of BOQ – e.g. if the doctors on duty were trained to handle HIV-related scenarios, and if people living with HIV are allowed to get more private consultation (instead of discussing the cases in public).
As of press time, however, NO RESPONSES WERE RECEIVED FROM BOTH GARIN AND SALCEDO.

BOQ’s Ferchito Avelino is hopeful that stakeholders “work together and disseminate information on HIV and correct myths that breed unnecessary fear that results to stigma and discrimination.”
On May 30, however, Ferchito L. Avelino, M.D. of the BOQ responded to Outrage Magazine, stating the bureau’s appreciation of “your effort to communicate to us your concerns. These information is important to us as we continue to improve client-to-doctor engagement (to) make sure that such engagement is within the bounds of medical confidentiality.”
Specific to the first concern raised by Outrage Magazine, Avelino stated that, “yes, the answer to the query on HIV status is based on self-disclosure of the client… although we strongly encourage client to disclose their status as this information is vital prior to the administration of any antigen. Also, our doctor may request the client to secure a certification from their attending physician on the needed for vaccination.”
(The HIV status is based on self-disclosure because of the confidentiality clause in the law – Ed)
Pertaining the possible breach in confidentiality that Xander noted in BOQ, Avelino stated that “aside from the doctor, (the) nurse on duty handles the information that are inputted in the BOQ form.” He added that “actions are made and continuously being updated to put in place systems and processes to make sure that other clients and service providers will have no access to this information.”
Avelino also stated that “the Bureau has medical doctors trained in internal medicine and in public health”, and that “to be updated on clinical practices, we conduct sessions in handling medical cases. In the past, we had sessions on HIV with representatives from the positive community.”
Avelino is hopeful that stakeholders “work together and disseminate information on HIV and correct myths that breed unnecessary fear that results to stigma and discrimination.”
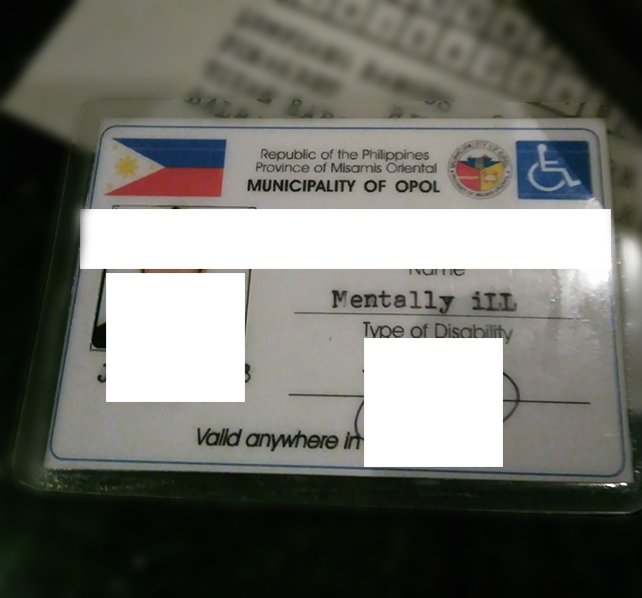
A person living with HIV (PLHIV) was given a PWD (person with disability) card by the City Social Welfare and Development (CSWD) that identified the bearer as a “PLHIV”. After a complaint was filed, the card was replaced; though the replacement now stated that the bearer of the ID is “mentally ill”.
While the BOQ is used here as a sample government office, it is – incidentally – not the only office (and a government office, particularly) that has issues when dealing with HIV-related cases.
Humphrey Gorriceta, a Filipino living with HIV, once recalled how he was “forced” to disclose his HIV status in the Land Transportation Office (LTO). Upon renewing his license in the LTO in Rosario, Cavite, Gorriceta had to take a drug test (a requirement).
“I just took my ARV about an hour or two before the testing (before giving my urine specimen), and the drug test result turned out positive. They asked me the routine questions if I have consumed alcohol recently or have taken any prohibited drugs. I said no. I asked why, and they said that they will have to send it to the DOH for confirmatory (drug test). I told them no need for that. I confessed that I am on ARV, and possibly the false-negative result is due to my ARV. I showed them my ARV caplets. They asked what ARVs are. I was surprised they didn’t know. I told them I have a lifetime condition that required me to take ARV, and that ARVs are like very strong antibiotics for a specific infection. They still didn’t get it and continued to ask about the meds. So I told them that ARVs are maintenance medication for HIV. I had to make the disclosure. I ended up explaining about HIV and ARV,” Gorriceta said.
Gorriceta added that he “felt it was uncalled for. I felt I was pushed against the wall to do the disclosure. For them to have a drug testing service means that they should be educated or at least be oriented of the possible scenarios why a person would come out (false) positive to drug testing.”
The mandatory drug testing for driver’s license applicants was scrapped after the Republic Act 10586 (Anti-Drunk and Drugged Driving Act) took effect in June 2013.
In another case, this time in Cagayan de Oro City (CDO), a person living with HIV (PLHIV) was given a PWD (person with disability) card by the City Social Welfare and Development (CSWD) that identified the bearer as a “PLHIV”. After a complaint was filed, the card was replaced; though the replacement now stated that the bearer of the ID is “mentally ill”.
For Stephen Christian Quilacio of the Northern Mindanao AIDS Advocates (NorMAA), this highlights “the lack of knowledge in handling an issue that continues to be very sensitive,” he said.
NorMAA now helps provide support to the CDO PLHIV.
“While we say that there is no shame in being HIV-positive, as it is supposed to be only a medical condition, we remain cognizant of the fact that society as a whole continues to not be accepting of PLHIV, who are often stigmatized and discriminated. Care should therefore be given in handling HIV-related cases; and this is not always provided even by those in government offices,” Quilacio said.
According to Ico Rodulfo, president and CEO of Project Red Ribbon, “discrimination among PLHIVs in government offices is still rampant. Project Red Ribbon has encountered a lot of reports and from personal experiences in the PLHIV community, where PLHIVs were bullied, not given chances to be promotion or are talked into quitting their posts. The Foundation also had an experience with one government agency which has an HIV program, but where the staff didn’t respect the confidentiality of the PLHIV and disclosed the status of the client to the neighborhood where she resides. This eventually caused her to be bullied and pressured to move out as her neighbors feared that her HIV might infect the entire barangay.”
CONFRONTING STIGMA AND DISCRIMINATION
Yet another example happened back in Cebu City, with the handling of the cadaver of a PLHIV who passed on. There, after the demise of the PLHIV, his family was allegedly told to “ilubong dayun ang patay kay basin makatakod (immediately bury the dead as it could infect others)”. His casket was also tightly wrapped in layers of plastic.
Outrage Magazine contacted the office of Dr. Ilya Tac-an, head of Cebu City’s Epidemiology Center and STD Detection Center, who said she will refer the publication to the one in charge with the cadaver section. Tac-an, nonetheless, stated that as far as she knows, the City Health Department is following the provision on the proper disposal of dead persons as mandated in the Presidential Decree 856, s. 1975, or the Code on Sanitation of the Philippines.
IRR of Chapter XXI (Disposal of Dead Persons) of PD 856, s. 1975, states that when the death due to “dangerous communicable diseases”, including HIV, the following are the requirements:
- The remains shall be buried within 12 hours after death;
- The remains shall not be taken to any place of public assembly;
- Only the adult members of the family of the deceased shall be permitted to attend the funeral;
- The remains shall be placed in a durable, air tight and sealed casket; and
- No permit shall be granted for the transfer of such remains.
As of press time, Outrage Magazine did not receive the referral from Tac-an.
However, according to Nenet Ortega, R.N., a licensed embalmer who is with the International Development Leadership and Learning Corporation now as one of its technical experts on health system strengthening/health sector reforms, as long as Universal Precautions (standard infection control guidelines) are followed, the risk of infection from a dead body is very low.
“Hindi naman gaya ng Scarlet Fever or diphtheria ang AIDS para ilibing (AIDS is not like Scarlet Fever or Diphtheria that requires for the body to be buried) within 24 hours. It also does not require hermetically sealed coffin,” Ortega said.
Ortega added that “TB, polio, hepatitis and HIV can effectively be killed by formaldehyde and other embalming chemicals. Also, embalmers are trained to protect themselves from getting any infection during embalming process. You know what, as long as there are no microorganism that is resistant to formaldehyde and other embalming fluids and chemicals, and as long as embalmers have the means to protect themselves, embalmers can and will always be able to serve the public.”
The fear of the dead PLHIV infecting others is also baseless, Ortega said. “Remember that the virus need a living cell as its host in order to replicate. When the body dies, all the cells die, so therefore the virus dies as well kasi patay na din ang mga white cells (because the white cells also die) within 24 hours. And by exposing it to formaldehyde earlier than 24 hours, the faster the cells are preserved, but the virus dies.”
Ortega added: “That incident in Cebu exposed the immediate family of the person who died to further stigma and discrimination. That action indirectly tells people na namatay ang taong nasa loob ng ataul na nakabalot pa ng plastic sa isang nakakahawa, nakakadiri at (that the person inside the coffin that is wrapped in plastic died from a contagious, disgusting and) fatal kind of disease.”
For Ortega, “that incident in Cebu is a gross discrimination. As if balutin ng plastic ang coffin (by wrapping the coffin in plastic) would be a protection enough to keep HIV. That is bullshit! Ignorance spreads stigmatization and discrimination, including ignorance of the simple Universal Precaution. And Universal Precaution is basic. It is practiced in all clinics, lying in, hospitals of all levels, in schools with anatomy, physiology, clinical and chemistry laboratories, in morgues, in all places where exposure to bodily fluids may happen.”
For Dr. Jose Narciso Melchor Sescon of the AIDS Society of the Philippines, “the City Health Office is handling and tracking these cases through the death certificate filed by relatives prior to the burial. Hospitals are required by DOH to report the types of infections borne as part of surveillance (PIDSR, or the Philippine Infectious Disease Surveillance Response). Take note what is discriminating is what you put in the death certificate and not necessarily the process or handling as there are funeral parlors highly competent to handle such cases (e.g. Funeraria Oro).”
For Sescon, “the reality is that not all funeral parlors are trained or are competent to handle bodies with infectious diseases. Yes, I agree that standard precautions must apply, but the reality is, not all abide by this. Add to this the reservations of the owners of embalming establishments if they are not trained to deal with such cases.”
In cases where there are no experts that can handle the cadaver of PLHIVs, “there are DOH memorandum or administrative orders that the city must follow that within 24 hours, the body should already be cremated or be buried. If only there are a lot of trained embalmers to handle highly infectious diseases, not only HIV but also the likes of meningococcemia and chicken pox, then it will not be a problem.”
Sescon added that “this may be why a PLHIV’s body had to be cremated or buried within 24 hours, particularly if there are no trained embalmers around, most especially in far-flung areas.”
He added, nonetheless, that “the manner of relaying the correct information is also important so that the situation is better understood.”
Both Ortega and Sescon advocate the further professionalization of the funeral industry for the people in it to know how to properly handle sensitive cases, such as when involving a dead PLHIV.
“I agree with the need to professionalize the profession for only then will this issue be somehow resolved. Professionalizing increases the quality standards of operations, provision of licenses and permit will depend now on meeting the quality standards in embalming bodies and or running a funeral parlor,” Sescon said.
RAMPANT STIGMA AND DISCRIMINATION
HIV-related stigma and discrimination has long been reported in the Philippines by the likes of Remedios AIDS Foundation and Pinoy Plus Association in a study called Exploring the Realities of HIV/AIDS Related Discrimination in Manila Philippines, published in 2005; APN+, Pinoy Plus Association and UNAIDS in AIDS Discrimination in Asia: From the Perspective of Persons Living with HIV/AIDS,
Published in 2002; and GNP+, Pinoy Plus Association and UNAIDS in The People Living with HIV Stigma Index in the Philippines, published in 2010.
These studies, in fact, note that the area where PLHIVs experience most discrimination is the healthcare setting (both public and private), with instances cited including: refusal to treat on the grounds of HIV status, different treatment on grounds of HIV status, testing for HIV without the knowledge of the individual, breach of confidentiality and denied of health insurance.
Eddy N. Razon of the Pinoy Plus Association, in his report AIDS Related Stigma and Discrimination in the Philippines, also noted the “non-availment of redress mechanisms” of PLHIVs. Among the reasons provided include: lack of understanding on what constitute human rights violations; lack of knowledge on available redress mechanism; unwillingness to come out and be identified in public in the course of seeking redress; and the cost of legal action.
And so – back to the access to the YF vaccine at the BOQ – Xander said it is a “Catch 22 situation. We’re damned if we disclose, and damned if we don’t disclose.”
In his case, Xander is first to admit the good of knowing how he may react to what will be injected into his body. He is now seeking medical clearance from his personal doctor, just so he can present some documentation to the BOQ.
But Xander said that he isn’t a “special case – there are others like me who also had YF vaccination, and who opted not to admit their HIV status just to be done and over with with the YF vaccination”.
And Xander said he understands the other PLHIVs, stressing that “unless protections are given to those who openly admit their HIV status, then expect PLHIVs to lie instead to protect themselves from stigma and discrimination.”
In CDO, NorMAA’s Quilacio believes in the need to revisit the approaches in the delivery of services of government offices, among others; though this time, “these need to be informed by the very people they claim to serve. Otherwise, if they persist as if it’s all business as usual, then they’re just going to continue doing things insensitively, and maybe even against the laws that ought to be upheld.”
Rodulfo said that “the challenges are aplenty. First, we need to educate the government offices and agencies about HIV and the law. Second, we need to implement the HIV in the workplace policy as required by RA 8504 and the DOLE mandate, so all government offices educate the workforce re respect of the rights of the workers with HIV. And third, we need to continue to push for anti-discrimination ordinances and policies.”
Rodulfo is, nonetheless, hopeful that change will come soon. “As change is coming with the next President, we are hopeful that reforms will be implemented to finally stop stigma and discrimination of members of the PLHIV community,” he said.
“We may still have a very long way to go when dealing with HIV-related issues,” admitted Xander. “But we’d have an even longer way to go if the very institutions that swore to uphold our rights – i.e. the government – are the very ones that violate them.” And so, “change needs to happen. And they need to happen fast.”
*THE INTERVIEWEE REQUESTED FOR HIS REAL NAME NOT TO BE USED TO PROTECT HIS PRIVACY
THIS IS A DEVELOPING STORY, AND OUTRAGE MAGAZINE WILL CONTINUE PURSUING LEADS THAT HIGHLIGHT NOT ONLY ERRONEOUS PRACTICES BUT BEST PRACTICES WHEN DEALING WITH HIV IN VARIOUS OFFICES





























